You are here
Thoughts On Chronic Shoulder Instability
Could you do an article on shoulders that pop out of the socket? I have one of those. When I lean forward, my left shoulder pops out of the socket and it's very painful and I can shove it back in. Do you think I need to see a doctor or is there something I could do to keep it from happening?
Thanks!
Mary M.
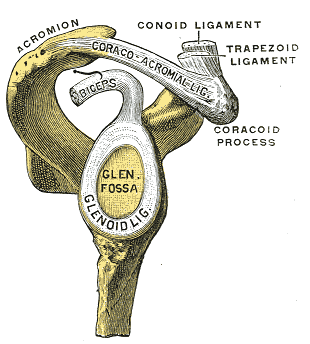 Mary is describing recurrent shoulder dislocations. The head of the humerus (arm bone) is held in the socket of the shoulder joint by a series of strong ligaments. These stabilizing ligaments attach themselves to a number of bony protuberances in and around the joint, as well as to the glenoid labrum (pictured here), which is a key ring of cartilage that acts almost like a suction cup and shock absorber that deepens the socket of the shoulder joint to cradle the ball of the humerus.
Mary is describing recurrent shoulder dislocations. The head of the humerus (arm bone) is held in the socket of the shoulder joint by a series of strong ligaments. These stabilizing ligaments attach themselves to a number of bony protuberances in and around the joint, as well as to the glenoid labrum (pictured here), which is a key ring of cartilage that acts almost like a suction cup and shock absorber that deepens the socket of the shoulder joint to cradle the ball of the humerus.
In many cases of a recurring shoulder dislocation, the labrum itself has partly detached from the bony socket to which it should stay anchored. When this is the case, in my experience, no amount of strengthening of surrounding muscles will prevent further dislocations unless a person is extremely mindful of avoiding overhead activities; even with great precaution, when the labrum is partially torn away from the socket of the scapula, one can expect recurrent dislocations.
Most specialists will staple the detached portion of labrum back into the bony socket and tighten the ligamentous capsule that is intended to keep the ball of the humerus from dislocating. Standard practice is to over-tighten to some degree to make the joint as stable as possible, and then to induce needed flexibility in the joint through post-surgery rehab.
My opinion is to consider the surgery and rehab route if your everyday activities involve having your arms out to your side or above your head. If you love playing a sport that requires full use of your shoulder, if you plan on having children and being active with them, if your work requires that you regularly reach out and up with your arms - these are a few examples of cases when I think it makes sense to seriously consider undergoing surgery.
If you can get by without putting your arms in compromising positions, then I would suggest doing the best you can with strengthening exercises for your rotator cuff muscles (subscapularis, infraspinatus, teres minor, and supraspinatus) and other surrounding muscles that can help stabilize the gleno-humeral joint to some degree - these larger muscles would be your lats and pecs; a physiotherapist or experienced fitness trainer can guide you through helpful strengthening exercises. The key position to avoid is having your arms raised while your shoulders are externally rotated as they would be if you sleep face up with your hands under your head.
In Mary's case, without evaluating her shoulder, it does sound like she has a tear of her glenoid labrum, something called a SLAP lesion. There are some drawbacks to going through surgery and rehab to repair a SLAP lesion, including a small risk of developing a neurological condition called reflex sympathetic dystrophy, but given the frequency and pain of her dislocations, I would think that the advantages of corrective surgery outweigh potential risks and the struggles of rehab.
Please note: If you have a shoulder that dislocates from time to time, it's best to avoid the internal rotation stretch found here: Internal Rotation Stretch for Shoulder Impingement.
Join more than 80,000 readers worldwide who receive Dr. Ben Kim's free newsletter
Receive simple suggestions to measurably improve your health and mobility, plus alerts on specials and giveaways at our catalogue


Please Rate This
Highest Rated | Related Posts | ||